BREAST RECONSTRUCTION
Breast reconstruction is usually employed after cancer surgery including mastectomy and breast conserving surgery. Following the radiotherapy when it is indicated and after prophylactic mastectomy in high risk patients.
The best time to think about breast reconstruction options is usually before the surgery in order to choose between an immediate or delayed reconstruction. Therefore sufficient information must be given to the patients in order to make an educated decision and choosing the most appropriate procedure or even choose not to have reconstructive surgery.
Although delayed reconstruction used to be preferred so that the patient would have the time to accept the loss of her breast before making a decision, recently a holistic treatment approach of breast cancer involves, which breast reconstruction immediately after the mastectomy, is becoming more preferable since it offers great psychological benefits and a better adjustment to the diagnoses. Breast reconstructive surgery lessens the psychological impact of breast cancer by eliminating the disfigurement and feeling of asymmetry following a mastectomy and can offer an improved body image and quality of life by decreasing anxiety and depression.
Following a holistic approach the patient can wake up with a mounted breast which can be psychologically beneficial since the patients will not have to deal with feelings of deformity and altered body image. Furthermore the surgeon has the opportunity to work with undamaged tissue since there is no fibroses and scar tissue which could affect the result of the reconstructive surgery and cause further discomfort to the patient.
Delayed reconstruction is performed in cases where the cost of an immediate reconstruction cannot be covered or if a patient has not decided if she wants to have reconstructive surgery. Some women may be advised to wait if they are having adjuvant radiotherapy following the surgery in order to give the skin a chance to recover from the effects of radiation.
A subpectoral breast reconstruction involves the implantation of silicone implants. The silicone implant consists of a silicone shell filled with a set amount of silicone which is inserted under the muscles laying over the chest wall (pectoralis major and parts of seratus anterior and rectus abdominis). This breast reconstruction is usually more fit for patients with small breasts.
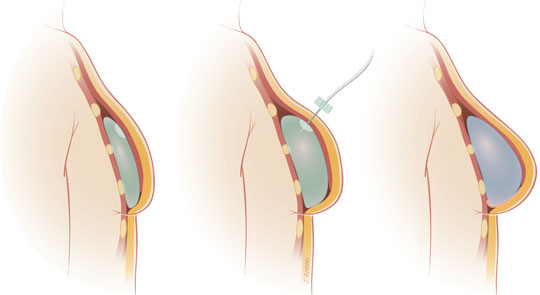
In patients with larger or ptotic breasts a tissue expander procedure may be used instead which can either be carried out as an immediate or delayed reconstruction. In this case a fluid filled sac, which can be inflated over weeks or months to stretch the skin and muscles, is inserted under the muscles and the expansion continues as an outpatient procedure, usually every week, in order to adjust the volume of the implant to much the other breast. If the patient has had radiotherapy this reconstruction may not be recommended since radiotherapy can cause extensive fibroses of the muscles and skin but if a tissue expander is already then the radiotherapy can still be carried out.
Breast reconstruction is usually employed after cancer surgery including mastectomy and breast conserving surgery. Following the radiotherapy when it is indicated and after prophylactic mastectomy in high risk patients.
The best time to think about breast reconstruction options is usually before the surgery in order to choose between an immediate or delayed reconstruction. Therefore sufficient information must be given to the patients in order to make an educated decision and choosing the most appropriate procedure or even choose not to have reconstructive surgery.
Although delayed reconstruction used to be preferred so that the patient would have the time to accept the loss of her breast before making a decision, recently a holistic treatment approach of breast cancer involves, which breast reconstruction immediately after the mastectomy, is becoming more preferable since it offers great psychological benefits and a better adjustment to the diagnoses. Breast reconstructive surgery lessens the psychological impact of breast cancer by eliminating the disfigurement and feeling of asymmetry following a mastectomy and can offer an improved body image and quality of life by decreasing anxiety and depression.
Following a holistic approach the patient can wake up with a mounted breast which can be psychologically beneficial since the patients will not have to deal with feelings of deformity and altered body image. Furthermore the surgeon has the opportunity to work with undamaged tissue since there is no fibroses and scar tissue which could affect the result of the reconstructive surgery and cause further discomfort to the patient.
Delayed reconstruction is performed in cases where the cost of an immediate reconstruction cannot be covered or if a patient has not decided if she wants to have reconstructive surgery. Some women may be advised to wait if they are having adjuvant radiotherapy following the surgery in order to give the skin a chance to recover from the effects of radiation.
A subpectoral breast reconstruction involves the implantation of silicone implants. The silicone implant consists of a silicone shell filled with a set amount of silicone which is inserted under the muscles laying over the chest wall (pectoralis major and parts of seratus anterior and rectus abdominis). This breast reconstruction is usually more fit for patients with small breasts.
In patients with larger or ptotic breasts a tissue expander procedure may be used instead which can either be carried out as an immediate or delayed reconstruction. In this case a fluid filled sac, which can be inflated over weeks or months to stretch the skin and muscles, is inserted under the muscles and the expansion continues as an outpatient procedure, usually every week, in order to adjust the volume of the implant to much the other breast. If the patient has had radiotherapy this reconstruction may not be recommended since radiotherapy can cause extensive fibroses of the muscles and skin but if a tissue expander is already then the radiotherapy can still be carried out.
In women who are having prophylactic mastectomy a subcutaneous breast reconstruction is usually performed. During this procedure the breast tissue is removed while the overlying skin, nipple and areola are preserved and a silicone implant is placed to fill the void. Subcutaneous breast reconstruction is usually not suggested to patients who have cancer since there is a risk of recurrence in the preserved nipple and skin.
Complications of breast reconstructive surgery using silicone implants may include discomfort due to the stretching of the skin and muscles, inflammation, swelling and formation of some scar tissue. Capsular contracture, which is formed by the contraction of the fibrous capsule that normally forms around the implant, can cause hardening and deformity of the breast and in those cases the implant is usually removed. Removal of the implant must also take place if the implant raptures and silicone ‘leaks’ into the surrounding tissues or in cases of infection. Finally silicone implants obscure X-rays and thus follow-up mammography will be more difficult to perform.
Myocutaneous tissue reconstruction
In this breast reconstructive procedure healthy tissue of the patient (flap) consisting of muscle, muscle with skin or muscle with skin and fat is moved to the chest to reconstruct the breast. There are two types of flaps:
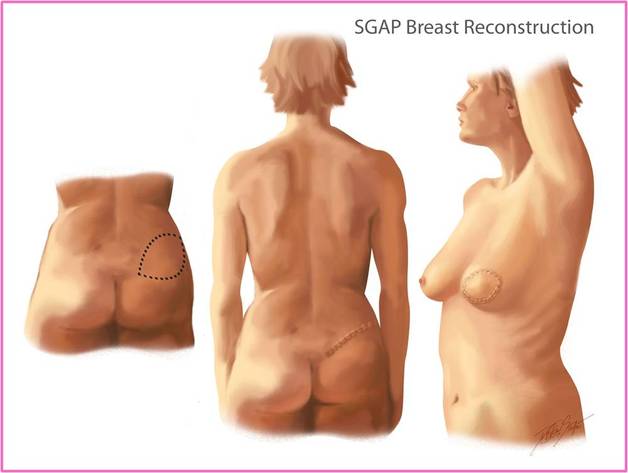
In a free tissue flap reconstruction the tissue is completely cut from the donor site and in order to be moved to the chest the blood supply is cut and the veins and arteries are reconstructed ta the new site. The free flap gives a good cosmetic result and has only a few complications even though it is a very complex long and technically difficult procedure. Gluteal flaps are always free due to the distance between the donor site and the chest and the small length of the gluteal vessels. Gluteal flaps are recommended only to women who have sufficient extra tissue in the gluteal area and used only as a last resort.
Complications of breast reconstructive surgery using silicone implants may include discomfort due to the stretching of the skin and muscles, inflammation, swelling and formation of some scar tissue. Capsular contracture, which is formed by the contraction of the fibrous capsule that normally forms around the implant, can cause hardening and deformity of the breast and in those cases the implant is usually removed. Removal of the implant must also take place if the implant raptures and silicone ‘leaks’ into the surrounding tissues or in cases of infection. Finally silicone implants obscure X-rays and thus follow-up mammography will be more difficult to perform.
Myocutaneous tissue reconstruction
In this breast reconstructive procedure healthy tissue of the patient (flap) consisting of muscle, muscle with skin or muscle with skin and fat is moved to the chest to reconstruct the breast. There are two types of flaps:
In a free tissue flap reconstruction the tissue is completely cut from the donor site and in order to be moved to the chest the blood supply is cut and the veins and arteries are reconstructed ta the new site. The free flap gives a good cosmetic result and has only a few complications even though it is a very complex long and technically difficult procedure. Gluteal flaps are always free due to the distance between the donor site and the chest and the small length of the gluteal vessels. Gluteal flaps are recommended only to women who have sufficient extra tissue in the gluteal area and used only as a last resort.
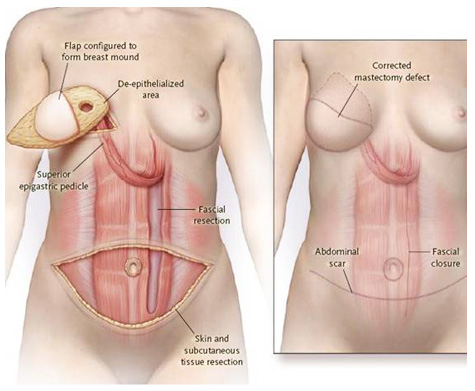
During a pedicle tissue flap reconstruction the skin fat and muscle are cut free from the donor site while preserving the blood supply and the flap is is moved nearby (only as far as the length of the blood vessels will allow). A pedicle tissue flap gives a good cosmetic result and is technically less difficult than the free tissue flap procedure and the surgery has more complications but they are easy to deal with. The myocutaneous flaps require movement of the latisimus dorsi muscle (muscle of the back) with overlying skin or the lower abdominal fat and skin based on the rectus abdominis muscle (TRAM flap) which can be used as a pedicle tissue flap.
After the reconstruction has healed and the breast has steeled into its final shape and position the nipple can be reconstructed to the correct position from grafted skin usually taken from the top of the inner thigh and the areola can be tattooed after the surgery. Another choice is to use prosthetic nipples which are stick on and in these cases the nipple can be made using a mould of the remaining nipple.
Some women prefer not to go through a breast reconstruction surgery and in this cases external breast forms or prostheses can be used to achieve a symmetrical result. Furthermore for women who are having delayed reconstructive surgery, a temporary breast prosthesis is used until the time comes to have the surgery. Finally special mastectomy bras, which are pocketed to keep the prosthesis stable, are available for women who decide not to have breast reconstruction.
Some women prefer not to go through a breast reconstruction surgery and in this cases external breast forms or prostheses can be used to achieve a symmetrical result. Furthermore for women who are having delayed reconstructive surgery, a temporary breast prosthesis is used until the time comes to have the surgery. Finally special mastectomy bras, which are pocketed to keep the prosthesis stable, are available for women who decide not to have breast reconstruction.