WHAT IS CANCER?
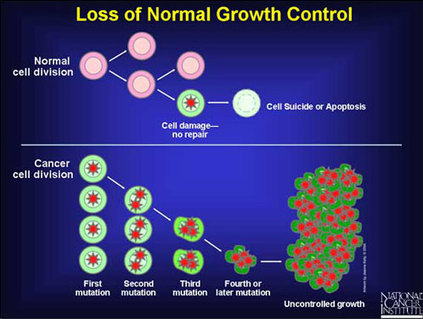
During development our cells divide and multiply rapidly to achieve increase of our body size. In the adult cells continue to multiply to substitute the dying cells but they do not act to increase the body size. The sensitive balance between dying cells and new cells being produced is maintained by the controlled division and programed death of cells. When a cell ‘loses’ control of its division and multiplies rapidly it can lead to the formation of a benign or malignant growth.
The cells life cycle and consequently its division and death rates are strictly controlled by special DNA sequences (genes). Therefore changes or mutations of those genes can lead to the out of control division of the cell and result to the formation of a mass. The cells have ‘defence’ mechanisms to protect their complex regulatory cycles and therefore a series of defences must be overcome for the regulatory cycle to become irregular. Most of the breast cancers similarly to other kinds of cancers cells carry mutable mutations which occur randomly over a long period of time.
From the above it is becoming clear that the main characteristic of cancer is the abnormal and uncontrolled cell division of a tissue which can invade and cause damage to the normal body tissue. A benign tumour consists of cells that do not invade the surrounding tissues and the damage it may cause is mostly attributed to the increased pressure on the surrounding tissues due to the increase of the cell mass. On the other hand a malignant tumour consists of cells that can invade surrounding tissues and migrate from the primary tumour to form secondary tumours (metastases) destroying distant tissues.
Breast cancer originates from the epithelium that covers the ducts (ductal carcinoma) or from the epithelium of the ducts that lie in the lobules (lobular carcinoma). Most ductal carcinomas are invasive, which means that they invade the tissues surrounding the ducts, while lobular carcinomas can be either invasive or in situ, which means that the cancer cells do not invade the surrounding tissues but rather remain confined in their place of origin.
During development our cells divide and multiply rapidly to achieve increase of our body size. In the adult cells continue to multiply to substitute the dying cells but they do not act to increase the body size. The sensitive balance between dying cells and new cells being produced is maintained by the controlled division and programed death of cells. When a cell ‘loses’ control of its division and multiplies rapidly it can lead to the formation of a benign or malignant growth.
The cells life cycle and consequently its division and death rates are strictly controlled by special DNA sequences (genes). Therefore changes or mutations of those genes can lead to the out of control division of the cell and result to the formation of a mass. The cells have ‘defence’ mechanisms to protect their complex regulatory cycles and therefore a series of defences must be overcome for the regulatory cycle to become irregular. Most of the breast cancers similarly to other kinds of cancers cells carry mutable mutations which occur randomly over a long period of time.
From the above it is becoming clear that the main characteristic of cancer is the abnormal and uncontrolled cell division of a tissue which can invade and cause damage to the normal body tissue. A benign tumour consists of cells that do not invade the surrounding tissues and the damage it may cause is mostly attributed to the increased pressure on the surrounding tissues due to the increase of the cell mass. On the other hand a malignant tumour consists of cells that can invade surrounding tissues and migrate from the primary tumour to form secondary tumours (metastases) destroying distant tissues.
Breast cancer originates from the epithelium that covers the ducts (ductal carcinoma) or from the epithelium of the ducts that lie in the lobules (lobular carcinoma). Most ductal carcinomas are invasive, which means that they invade the tissues surrounding the ducts, while lobular carcinomas can be either invasive or in situ, which means that the cancer cells do not invade the surrounding tissues but rather remain confined in their place of origin.
RISK FACTORS
Genetic predisposition
It has been shown that only 5-10% of breast cancers are affiliated with an autosomal dominant pattern of inheritance. Most breast cancers are a result of random changes of the breast tissue cells that can be caused during a long period of time. Women with family history of breast cancer have more chances of developing breast cancer. The risk varies according to the age and the number of the relatives that presented with the disease. However mutations on two genes called BRCA1 and BRCA2 have been shown to contribute to the development of cancer. It is speculated that the BRCA1/2 wild-type alleles (normal) play a role in suppressing developing tumours and that thoe genes are involved in the DNA repair mechanisms which take place right after the duplication of the DNA and constitute the main mechanism of avoiding mutations to ‘pile-up’ during duplication of DNA.
Age
Breast cancer is closely linked with age and the risk of developing breast cancer increases rapidly after the age of 45. Even though breast cancer is rare in young women, in cases when cancer is diagnosed in women under the age of 35, there are more chances that the cancer will be aggressive and the disease is caused usually by cancer susceptibility gene.
Hormonal risk factors
The total length of menstruation, including early age of menstruation and late age of menopause, contributes to a higher risk of developing breast cancer. Furthermore postmenopausal oestrogen replacement therapy has been linked to increased risk which is even higher when it exceeds 15 years of treatment. On the other hand use of contraceptives does not appear to increase the risk of exogenous exposure to oestrogen varies according to age.
Finally nulliparous women have a higher risk of developing the disease than parous women. Furthermore the age of parity also seems to play a role in increased risk of developing breast cancer. Studies have shown that if the first live birth is after the age of 35 the risk of developing breast cancer is equal or higher to that of nulliparous women whereas early first live birth, especially before the age of 20, seems to provide a degree of protection from the disease.
Diet
Total caloric intake and increased body fat have been shown to increase the risk of mammary cancer in animals. There is a positive association between cancer and obesity especially in postmenopausal women. It has been proposed that increased body fat increases the availability of endogenous oestrogens and/or changes the concentration of steroid hormones in the plasma.Finally there is a weak association between breast cancer and alcohol consumption.
Radiation exposure
The data collected from women exposed to Hiroshima and Nagasaki atomic bombs have proved there is an association between increased risk for breast cancer and radiation exposure. Furthermore it has been shown that the risk of developing the disease is also increased in cases where X-rays have been used as a diagnostic treatment tool. In those cases the age of exposure also pays an important role with women exposed during puberty being at greatest risk.
Mammographic density
It has been shown that increased mammographic density increases the chances of developing breast cancer.
Genetic predisposition
It has been shown that only 5-10% of breast cancers are affiliated with an autosomal dominant pattern of inheritance. Most breast cancers are a result of random changes of the breast tissue cells that can be caused during a long period of time. Women with family history of breast cancer have more chances of developing breast cancer. The risk varies according to the age and the number of the relatives that presented with the disease. However mutations on two genes called BRCA1 and BRCA2 have been shown to contribute to the development of cancer. It is speculated that the BRCA1/2 wild-type alleles (normal) play a role in suppressing developing tumours and that thoe genes are involved in the DNA repair mechanisms which take place right after the duplication of the DNA and constitute the main mechanism of avoiding mutations to ‘pile-up’ during duplication of DNA.
Age
Breast cancer is closely linked with age and the risk of developing breast cancer increases rapidly after the age of 45. Even though breast cancer is rare in young women, in cases when cancer is diagnosed in women under the age of 35, there are more chances that the cancer will be aggressive and the disease is caused usually by cancer susceptibility gene.
Hormonal risk factors
The total length of menstruation, including early age of menstruation and late age of menopause, contributes to a higher risk of developing breast cancer. Furthermore postmenopausal oestrogen replacement therapy has been linked to increased risk which is even higher when it exceeds 15 years of treatment. On the other hand use of contraceptives does not appear to increase the risk of exogenous exposure to oestrogen varies according to age.
Finally nulliparous women have a higher risk of developing the disease than parous women. Furthermore the age of parity also seems to play a role in increased risk of developing breast cancer. Studies have shown that if the first live birth is after the age of 35 the risk of developing breast cancer is equal or higher to that of nulliparous women whereas early first live birth, especially before the age of 20, seems to provide a degree of protection from the disease.
Diet
Total caloric intake and increased body fat have been shown to increase the risk of mammary cancer in animals. There is a positive association between cancer and obesity especially in postmenopausal women. It has been proposed that increased body fat increases the availability of endogenous oestrogens and/or changes the concentration of steroid hormones in the plasma.Finally there is a weak association between breast cancer and alcohol consumption.
Radiation exposure
The data collected from women exposed to Hiroshima and Nagasaki atomic bombs have proved there is an association between increased risk for breast cancer and radiation exposure. Furthermore it has been shown that the risk of developing the disease is also increased in cases where X-rays have been used as a diagnostic treatment tool. In those cases the age of exposure also pays an important role with women exposed during puberty being at greatest risk.
Mammographic density
It has been shown that increased mammographic density increases the chances of developing breast cancer.